-
How does Dr. Buonassisi decide which rhinoplasty technique to use?
The technique is never decided in advance. Dr. Buonassisi assesses your nasal anatomy — skin thickness, cartilage strength, septum structure, and the specific changes you want to achieve — and recommends the approach most likely to produce a natural, lasting result for your case. There is no single technique that suits every patient, and no technique that is automatically superior. The surgical plan is built around your anatomy, not around a preferred method.
-
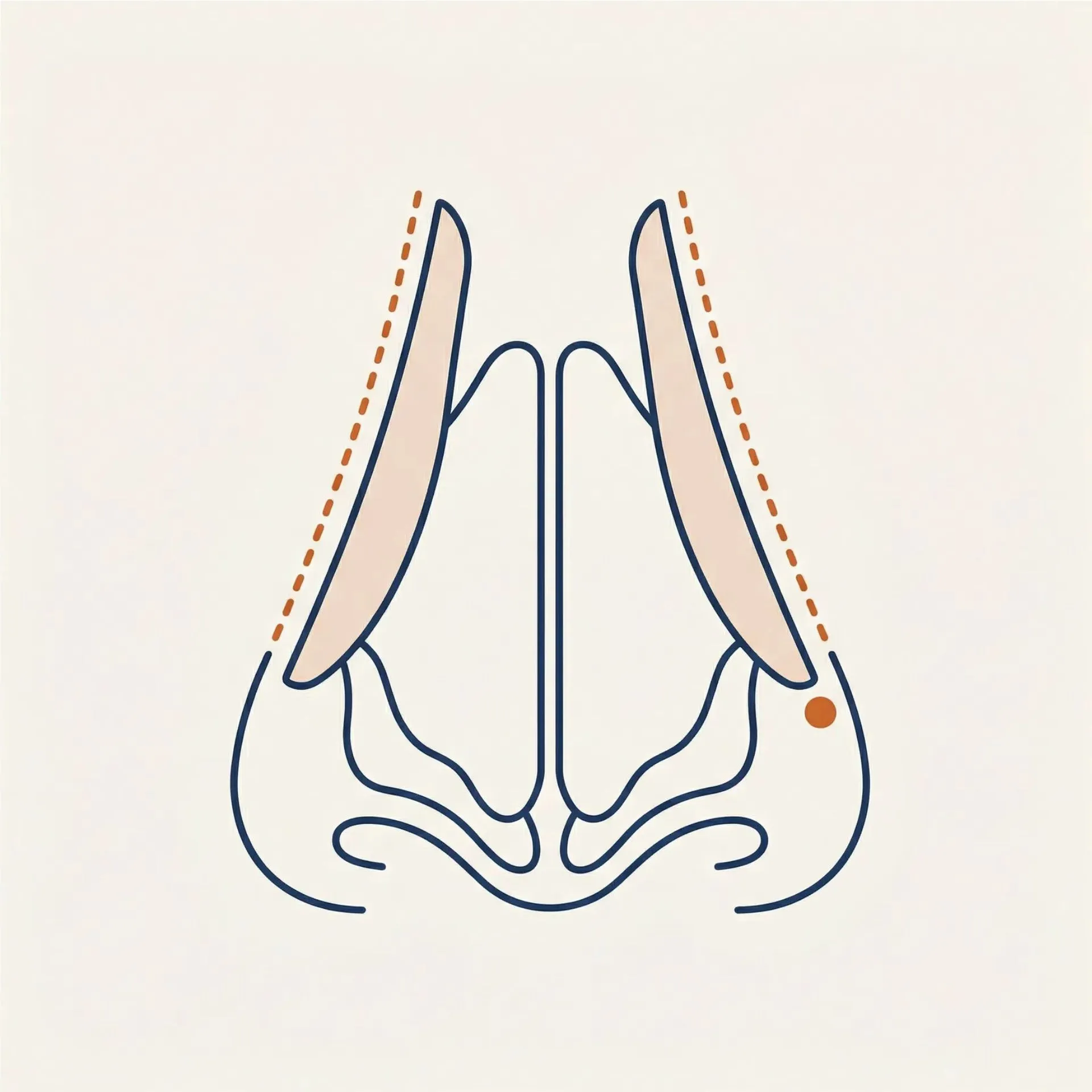
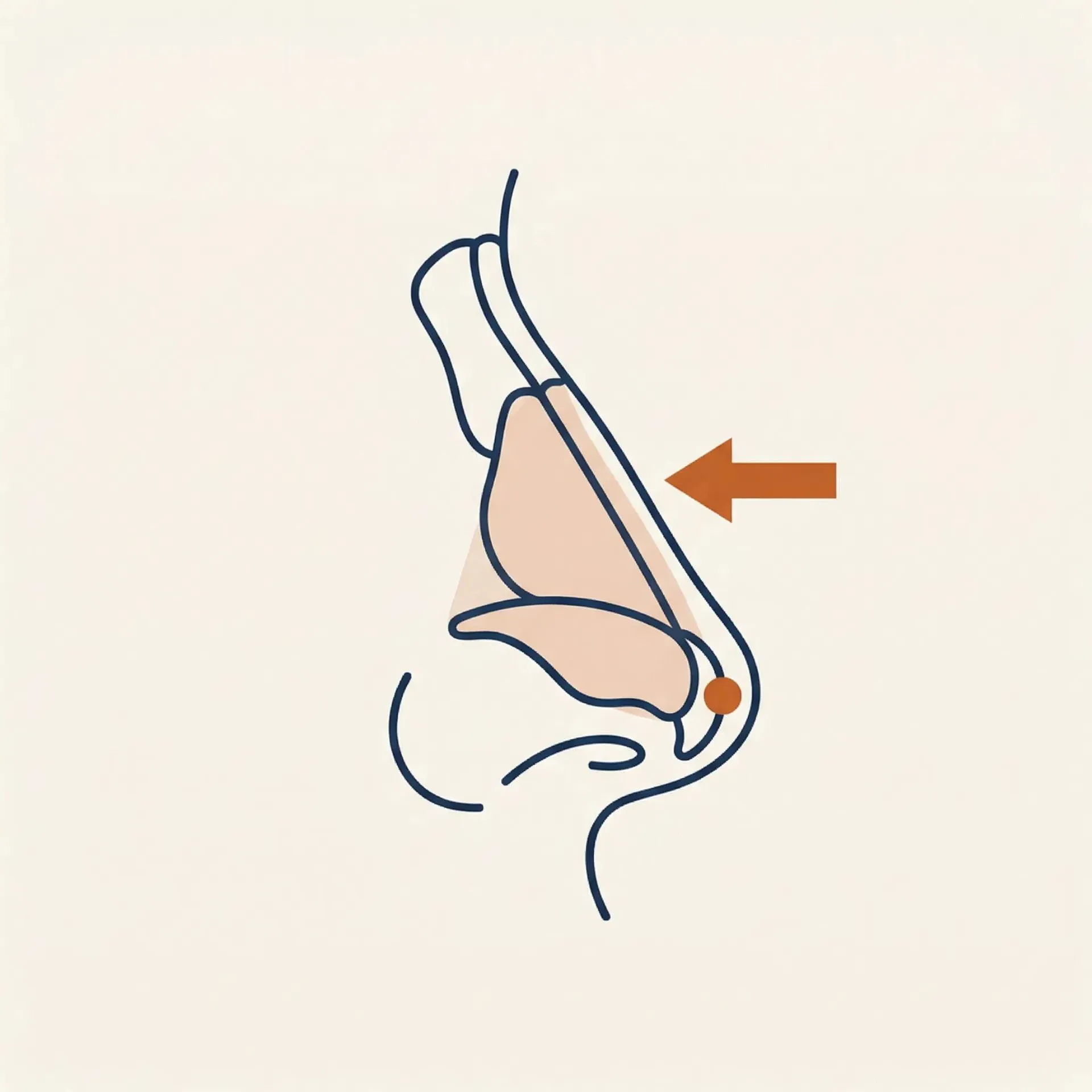
What is preservation rhinoplasty and how is it different from traditional rhinoplasty?
Preservation rhinoplasty reshapes the nose by conserving the native nasal bridge and key ligaments rather than removing and rebuilding them. In a traditional approach, the dorsal hump is excised from above — which requires rebuilding the middle vault afterwards. In preservation, the bridge is lowered from beneath while the overlying tissue remains intact. The result is a smoother, more natural-looking profile with typically less post-operative swelling and bruising. It is not the right approach for every patient — Dr. Buonassisi evaluates whether your cartilage strength and anatomy are suitable before recommending it.
-
Is open or closed rhinoplasty better?
Neither approach is universally better — the right choice depends on your anatomy and the complexity of what needs to be achieved. Open rhinoplasty uses a small incision across the columella to give the surgeon full visibility of the nasal structure. It is preferred for complex cases, significant tip work, and revision surgery. Closed rhinoplasty is performed entirely through internal incisions with no external scar, and suits more limited changes. Dr. Buonassisi will recommend the appropriate approach at your consultation based on what your specific goals require.
-
Can hump reduction be done on its own, or does the tip always need to be addressed at the same time?
In most cases, hump reduction and tip work are planned together. Lowering the nasal bridge changes the proportions of the entire nose — a reduced bridge with an unchanged tip can look disproportionate. The tip almost always needs to be considered at the same time to ensure the result looks balanced from every angle, not just in profile. There are cases where the tip is already well-proportioned and requires little or no adjustment, but this is assessed individually — it is not assumed.
-
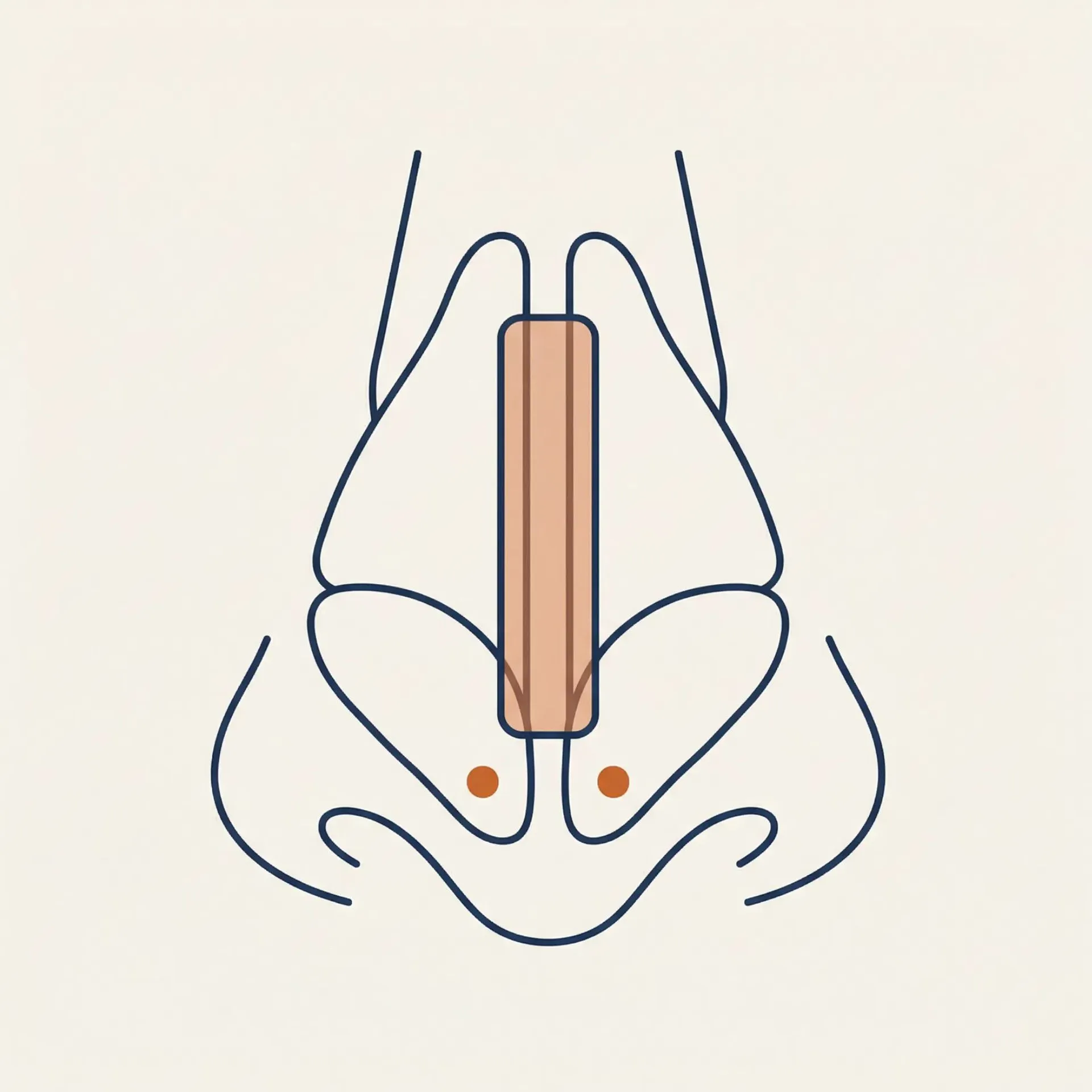
Can rhinoplasty be combined with septoplasty?
Yes. Septoplasty — to straighten a deviated septum and restore natural airflow — is frequently performed at the same time as cosmetic rhinoplasty. This is called a septorhinoplasty. Combining the procedures means a single recovery period. The septum also serves as the primary donor site for cartilage grafts used in structural reconstruction, so correcting a deviation often provides material that supports the cosmetic work. At 8 West Clinic, septoplasty is performed as part of the rhinoplasty procedure — not as a standalone operation.
-
What is ethnic rhinoplasty and how does Dr. Buonassisi approach it?
Ethnic rhinoplasty is a specialised approach that refines and balances the nose while preserving the patient's cultural and ethnic identity. The goal is never to make a nose look less ethnic — it is to refine it in a way that honours the patient's heritage and facial structure. A standard one-size-fits-all approach can erase characteristics that are meaningful to the patient and produce a result that looks out of place. Dr. Buonassisi starts from your anatomy and your own definition of balance, and selects techniques — such as bridge augmentation, alar base reduction, or tip refinement — that enhance your features without imposing a different aesthetic standard.
-
Can Dr. Buonassisi correct a rhinoplasty performed by another surgeon?
Yes — though Dr. Buonassisi accepts revision cases selectively. Revision rhinoplasty is one of the most technically complex procedures in facial surgery — scar tissue alters the anatomy, native cartilage is often depleted, and the structural integrity of the nose may be compromised. He conducts a detailed clinical assessment to determine what is structurally present, what is realistically achievable, and whether ear or rib cartilage grafts will be needed. He provides an honest assessment of the complexity of your case, including what can and cannot be corrected, and will decline to proceed if the case is not one he can meaningfully improve. Patients considering revision are encouraged to complete the pre-assessment before booking a consultation.
-
Can teenagers have rhinoplasty?
Rhinoplasty for younger patients is considered once facial growth is complete — typically around 15–16 for girls and 17–18 for boys, once growth plates have closed. The procedure uses the same techniques as adult rhinoplasty; what differs is the assessment process. Dr. Buonassisi takes a conservative approach with younger patients: he assesses growth completion, discusses motivations candidly with both the patient and their family, and will decline to proceed if he has any concern about readiness or external pressure. A parent or guardian must be present at all consultations and must consent to the procedure.
-
What is ultrasonic rhinoplasty and when does Dr. Buonassisi use it?
Ultrasonic rhinoplasty uses a piezoelectric device — the piezotome — to sculpt nasal bone using high-frequency ultrasonic energy rather than traditional chisels and rasps. The instrument cuts bone precisely while leaving the surrounding soft tissue largely undisturbed, which typically results in less bruising and a faster recovery. Dr. Buonassisi uses the piezotome selectively — when the surgical plan includes bone-level changes and the patient's anatomy would benefit from its precision. It is not used as a default, and not every rhinoplasty requires bone work.
-
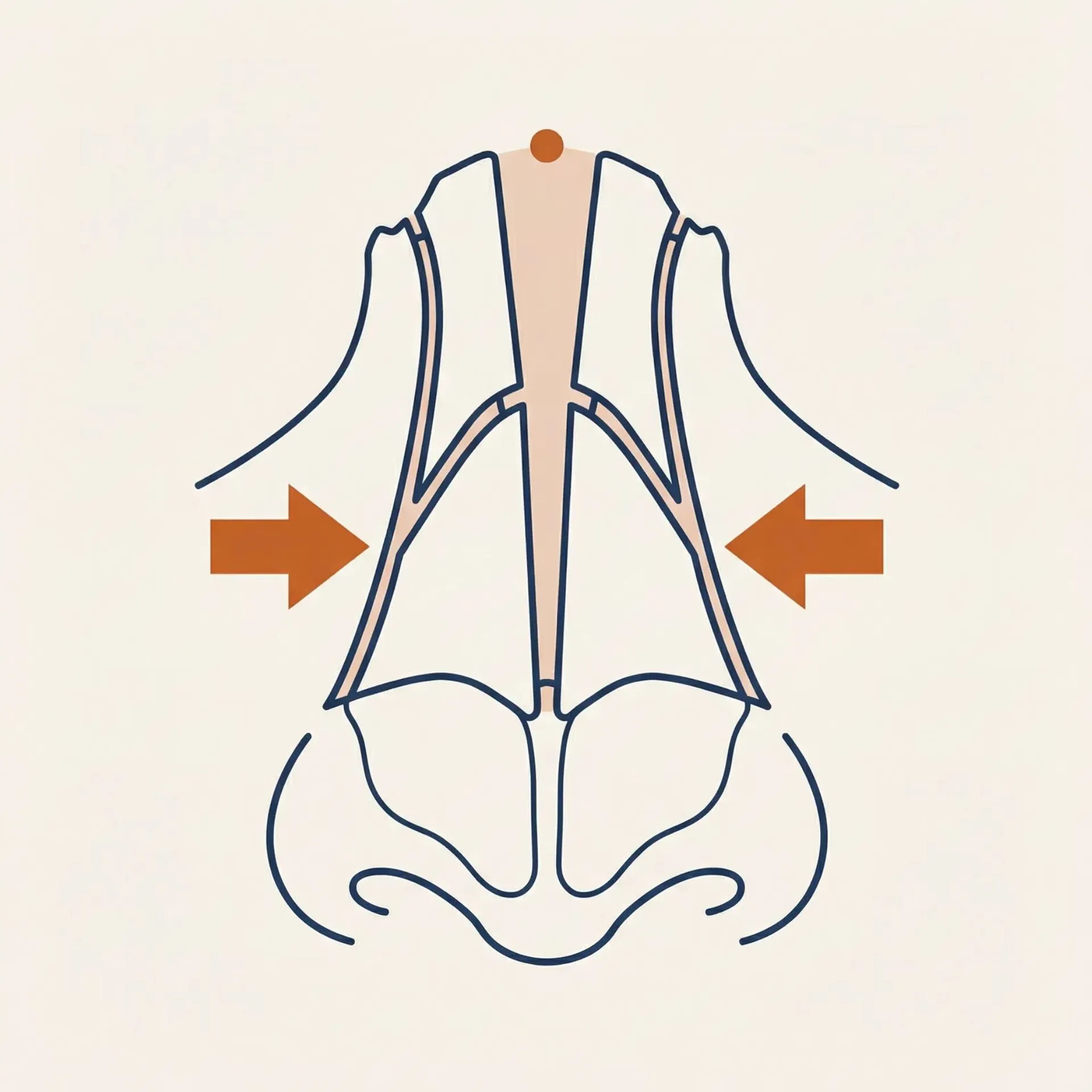
What does rhinoplasty involve as part of facial feminization surgery?
Rhinoplasty as part of facial feminization focuses on creating a softer, more feminine nasal profile. This typically involves narrowing the nasal bridge, refining the tip, reducing a dorsal hump if present, and slightly rotating the tip upward. The nose is central to facial gender perception — a bridge that reads as wide or a tip that reads as prominent can affect the overall feminization result even when other features have been addressed. Dr. Buonassisi plans nasal refinement as part of the broader facial balance, assessing which changes will have the most meaningful impact in the context of the patient's overall goals.
-
How long does rhinoplasty surgery take?
Surgery typically takes 1–3 hours depending on the complexity of the procedure and the technique used. Preservation rhinoplasty and closed rhinoplasty tend to be shorter. Complex open rhinoplasty, revision cases, and procedures combined with septoplasty may take longer. Dr. Buonassisi will give you a more specific estimate once your surgical plan has been determined.
-
What happens at a rhinoplasty consultation with Dr. Buonassisi?
Dr. Buonassisi conducts a detailed clinical assessment of your nasal anatomy — examining skin thickness, cartilage strength, septum structure, and the specific changes you want to achieve. Computer imaging is an important part of the process: it allows Dr. Buonassisi to show you what is realistically achievable for your anatomy and helps set accurate expectations before any decision is made. He will explain which techniques are appropriate for your case and what the outcome is likely to look like. He does not recommend a technique before assessing your anatomy, and he will not proceed if he has any concern about candidacy or expectations. The pre-assessment form, completed before your consultation, helps him prepare and ensures the appointment is focused on your specific case.
-
What is the recovery like after rhinoplasty?
Most patients experience swelling and bruising in the first 1–2 weeks. A splint is worn for approximately one week. The majority of visible swelling resolves within 4–6 weeks, though final results — particularly tip definition — continue to refine over 12 months as residual swelling subsides. Recovery varies depending on the technique used: preservation rhinoplasty and closed rhinoplasty typically involve less bruising and swelling than open or revision cases. Dr. Buonassisi's team provides detailed post-operative instructions and is available throughout recovery.
-
Is non-surgical rhinoplasty an option?
Non-surgical rhinoplasty uses injectable filler to temporarily adjust the appearance of the nose — smoothing a small bump, lifting the tip slightly, or improving symmetry. It is not a substitute for surgical rhinoplasty and cannot reduce the size of the nose or address structural concerns. Results are temporary. At 8 West Clinic, non-surgical rhinoplasty is offered for appropriate candidates who want a temporary improvement or want to preview a change before committing to surgery. It is not suitable for every concern — candidacy is assessed at consultation.
Results vary. This content is for informational purposes only and does not constitute medical advice. Book a consultation with Dr. Buonassisi to discuss your individual candidacy.